
Chronic Heart Failure (CHF) is a progressive, taxing condition that requires meticulous, daily management to prevent life-threatening exacerbations. For patients living in urban centers, access to specialized cardiology clinics is often a matter of a short drive. However, for those in rural “healthcare deserts,” the geography of care is much more treacherous. Patients in remote areas often face two-hour commutes to see a specialist, leading to deferred care, late-stage diagnoses, and significantly higher rates of hospital readmissions.
Remote Patient Monitoring (RPM) is emerging as the technological bridge for this divide. By utilizing non-invasive digital tools to transmit physiological data from a patient’s home to a clinical team in real-time, RPM effectively brings the cardiologist’s eyes into the rural living room.
The Clinical Challenge: The Rural Heart Failure Crisis
Rural populations often skew older and face higher rates of comorbidities like hypertension and Type 2 Diabetes. When these factors intersect with a shortage of local cardiologists, the result is a reactive rather than proactive care model. In heart failure management, the “Golden Window” for intervention occurs when a patient begins to retain fluid—long before they experience the acute shortness of breath that leads to an Emergency Room visit.
In a traditional rural setup, a patient might not realize they have gained five pounds of fluid until they are in respiratory distress. RPM changes this paradigm by shifting the focus from episodic office visits to continuous physiological oversight.
The RPM Ecosystem: How the Technology Works
An effective RPM program for heart failure is not just about a single device; it is an integrated ecosystem consisting of hardware, cellular connectivity, and clinical triage software.
- The Hardware Suite: A standard rural HF kit typically includes a Bluetooth or cellular-enabled weight scale, a blood pressure cuff, and a pulse oximeter. In more advanced cases, wearable ECG patches or necklaces can monitor heart rate variability and arrhythmias.
- Data Transmission: To overcome the “Digital Divide,” many modern RPM devices do not rely on home Wi-Fi, which can be spotty in rural areas. Instead, they use built-in SIM cards that transmit data via cellular networks as soon as the patient takes a measurement.
- The Clinical Hub: The data is sent to a secure cloud platform where AI-driven algorithms triage the results. If a patient’s weight increases by more than three pounds in 48 hours, an “Alert” is triggered, notifying a nurse or cardiologist to intervene.
Physiological Indicators: Detecting the “Silent” Exacerbation
The power of RPM lies in its ability to track “bio-signals” that the patient cannot feel.
- Sudden Weight Gain: This is the primary indicator of pulmonary edema (fluid in the lungs). Detecting this 48–72 hours before symptoms appear allows doctors to adjust diuretic medication over the phone, preventing a hospital stay.
- Blood Pressure Volatility: Chronic hypertension strains the heart muscle. Constant monitoring ensures that medications are titrated to the perfect dose for the patient’s daily environment, not just their “white coat” reading in a doctor’s office.
- Oxygen Saturation ($SpO_2$): For patients with concurrent COPD or advanced HF, tracking oxygen levels helps differentiate between heart-related breathlessness and respiratory issues.
Comparing Care Models: Traditional vs. RPM-Enhanced
The impact of RPM on rural care is best understood by comparing it to the standard episodic model.
| Feature | Traditional Rural Care | RPM-Enhanced Care |
| Detection of Fluid Retention | Patient notices breathlessness (Late) | Scale detects weight gain (Early) |
| Travel Burden | High (Frequent 50+ mile trips) | Low (Most care handled at home) |
| Hospital Readmissions | High (Reactive ER visits) | Low (Proactive medication tweaks) |
| Patient Engagement | Low (Disconnected between visits) | High (Daily awareness of metrics) |
Overcoming Barriers: The Digital Divide and Literacy
While the benefits are clear, implementation in rural areas faces significant hurdles:
- The Connectivity Gap: While cellular chips help, “dead zones” still exist. The expansion of satellite internet services like Starlink and the deployment of rural 5G are becoming essential components of modern healthcare infrastructure.
- Digital Literacy: Many rural CHF patients are elderly and may be intimidated by technology. Successful programs utilize “zero-config” devices—scales that work simply by being stepped on—and provide dedicated “tech-nurses” to walk patients through the initial setup via telephone.
- Reimbursement Models: Historically, doctors were only paid for face-to-face visits. However, the Center for Medicare & Medicaid Services (CMS) has introduced specific CPT codes (e.g., 99453, 99454) that allow clinics to be reimbursed for the time spent monitoring remote data, making the model financially viable for small rural practices.
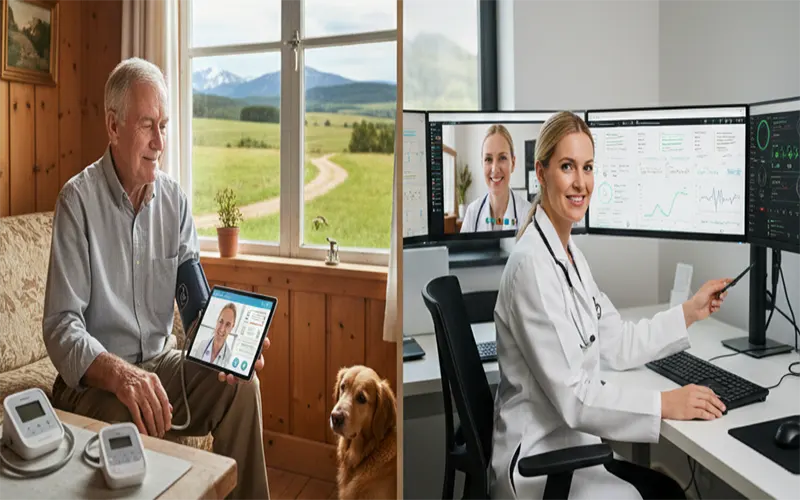
The Human Element: Telehealth and the “Local” Connection
It is a common misconception that RPM replaces the doctor-patient relationship. In reality, it strengthens it. When a rural patient sees their doctor via a telehealth screen, the doctor isn’t just asking “How do you feel?” Instead, the doctor is saying, “I see your blood pressure has been stable for two weeks, but your weight spiked yesterday. Let’s talk about your salt intake or adjust your Lasix.”
This data-driven conversation builds trust. The patient feels “seen” even though they are miles away, and the physician has the objective evidence needed to make safe, remote clinical decisions.
The Future of Rural Cardiology
Remote Patient Monitoring is the key to achieving health equity for rural populations. By transforming the home into a site of active clinical surveillance, we can strip away the “distance tax” that has long penalized rural heart failure patients.
As sensors become more sophisticated—moving into the realm of wearable “biochemical” sensors and advanced AI predictive analytics—the need for rural patients to travel for routine management will continue to dwindle. The future of heart failure management is not found in bigger hospitals, but in smarter, connected homes that allow patients to age in place with the security of a virtual cardiology ward watching over them.


